

Do you have good teeth contact (occlusion) ? or Do you have jaw joint disorder ?
What is teeth contact(occlusion)? What are they different between teeth contact and teeth alignment? Doesn't teeth contact really relate to TMJ disorder ?
目次
- Quite often teeth contact is determined only by your gut feeling and alignment of your front teeth though, people are usually unaware of only four types of bad occlusion.
- Occlusion is like examining if the hinge axis of the jaw joint shift or shake during chewing because occlusion always have to be in harmony with the hinge axis of jaw joint.
- Three sacred tools to prove if your occlusion is ideal.
- In this examination how to take an imprint of teeth contact on a sheet wax is most important because occlusion always have to be in harmony with the hinge axis of jaw joint.
- The big misconception about occlusion (teeth contact).
- What is teeth contact(occlusion)? What are they different between teeth contact and teeth alignment?
- Door hinge analogy for understanding teeth contact so much. When you see the door of a house, think of it as teeth contact.
- There are only four types of bad occlusion that people are usually not aware of though quite often teeth contact is determined only by your gut feeling and alignment of your front teeth.
- Seif-introduction
Quite often teeth contact is determined only by your gut feeling and alignment of your front teeth though, people are usually unaware of only four types of bad occlusion.
Various researches suggest that nine out of ten people originally have any of the four types of bad occlusion or teeth contact, but they are usually
unaware of them. In addition, you might have never seen any evidence showing your occlusion to be an ideal one.
There is a possibility your occlusion was determined based only on your own gut feeling and good alignment of front teeth,
but you may not be aware of the several types of bad occlusion.
I have a question for you. Do you have good occlusion or teeth contact? If you would say YES, what is your proof? Is it because you don’t feel anything
strange or difficult when chewing? Or did your dentist show you any evidence from an examination after your treatment?
If you’ve undergone orthodontic treatment, what you are shown as evidence of having good occlusion is so important because there are
cases where orthodontic treatment in dental practice caused the patients’ teeth and jaw joint to get damaged easily.
In my long experience I usually show my patients the evidence that their occlusion is ideal.
I’ll introduce a video of me showing a patient the evidence of good occlusion through a treatment of jaw joint disorder.
In this video, I will also introduce the two types of bad occlusion(①Not all teeth are in contact at the same time
②When grinding, molar teeth hit each other )in the four types of them that you are usually unaware of. These bad occlusions lead to tooth loss and jaw joint disorder.
Occlusion is like examining if the hinge axis of the jaw joint shift or shake during chewing because occlusion always have to be in harmony with the hinge axis of jaw joint.
Thank you for watching the video. What I would like to say is that occlusion is like examining if the hinge axis of the jaw joint shift or
shake during chewing. Dentists have to check if there is a leverage or see-saw movement when patients chew or grind their teeth with a method like this. Only this method can show evidence of good or bad occlusion. Chewing (during eating)and grinding the teeth (during sleeping)are natural processes of
our daily lives. So, if your occlusion has a leverage or seesaw movement, it gradually damages your teeth and jaw joint/ and lead to gum disease, tooth
fracture that require extraction, and jaw joint disorder. The more you chew and grind your teeth, the more your teeth and jaw joint will be damaged.
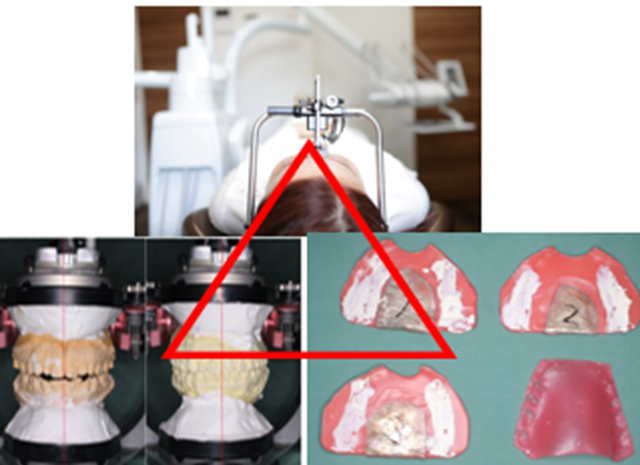
Three sacred tools to prove if your occlusion is ideal.
I always use three important tools when I show a patient the evidence whether they have good occlusion. I personally call them my three sacred tools.
First is a tool called facebow, a U-shape clamp with ear rods and it is put on you like the earpiece of stethoscope. Its function is to transfer functional
and aesthetic components from the mouth to another tool called dental articulator. This dental articulator allows the dentist to diagnose if an occlusion
has a leverage and whether the hinge axis of jaw joint shifts or shakes during chewing or grinding. In this examination how to take an imprint of
teeth contact on a sheet wax is most important because occlusion always have to be in harmony with the hinge axis of jaw joint. It means that when
chewing, the hinge axis of jaw joint should only rotate but doesn’t shift or shake. If it shifts or shakes, the leverage will eventually cause jaw joint disorder. The slightly higher molar tooth even by just a few millimeter acts like the fulcrum of a seesaw. This can cause progressive gum disease or teeth fracture
that may lead to tooth extraction. Therefore, we have to take an imprint of teeth contact on a sheet wax to determine whether the hinge axis of the jaw
joint only rotates and not even a bit of shifting or shaking.
In this examination how to take an imprint of teeth contact on a sheet wax is most important because occlusion always have to be in harmony with the hinge axis of jaw joint.
Can you remember the instructions from your dentist/ when he took an imprint to check your occlusion?
To help you remember, you can choose from the list below,
①Did your dentist ask you to open and close your mouth like you normally do, while using impression material.
②Did the dentist instruct you to bite firmly on a sheet of wax ?
③Did the dentist instruct you to relax your lower jaw, then they gently guided your lower jaw as you were closing your mouth until your upper and lower
teeth got in contact with sheet wax?
If it was ① or ②, your occlusion was determined based only by your habitual position or your gut-feeling.
If it was ③, your occlusion was determined based on the condition of the hinge
axis of your jaw joint. Finally, your occlusion harmonizes with the hinge axis of your jaw joint.
If it was ③, it is better to take three sheet wax imprints of teeth contact because if it’s only one or two imprints, there is no way to confirm its accuracy; but if there’s three, at least 2 are the same, and this will show the real occlusion.
The big misconception about occlusion (teeth contact).
One misconception even by many ordinary dentists is that teeth alignment and tooth contact are one and the same thing, but actually they are not.
Often, the dentist checks your teeth alignment by asking you to make teeth imprints by biting on a sheet wax or impression material.
From there they conduct their treatment. However, they don’t check leverage (see-saw movement) with the three sacred tools I called,
which occur during eating meals and griding at night in your daily life. Perhaps, they haven’t fully appreciated the impact of tooth contact and
TMJ movement on the overall dental health that’s why many cases of this problem remain unchecked. But the reality is tooth contact or occlusion is like
dentistry itself. Because if you have bad occlusion, the more you chew and grind your teeth, the more your teeth and jaw joint will be damaged.
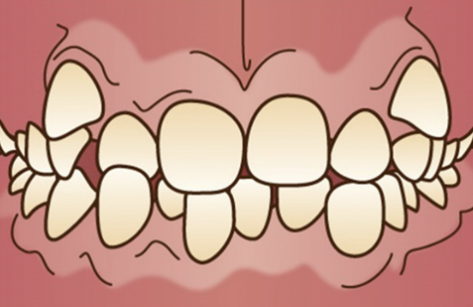
Unfortunately, this is not yet a widely recognized area of dental health. And quite often teeth contact is determined only by your gut feeling and
alignment of your front teeth though, people are usually unaware of bad occlusion. Improving the alignment of front teeth as shown below does not mean improving directly the teeth contact(occlusion) !From the top, Buck teeth, Under bite, Open bite, Vampire tooth.



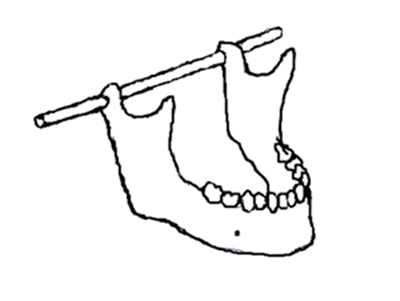
What is teeth contact(occlusion)? What are they different between teeth contact and teeth alignment?
So, let’s understand what is occlusion or good teeth contact? In my studies and years of experience in this profession, tooth contact is considered good when the hinge axis of jaw joint doesn’t shift or shake when you chew or grind your teeth. The hinge axis is most critical part of teeth occlusion
because it is the starting point of teeth contact. And it determines where the lower jaw teeth exactly contact with the upper jaw teeth.
Awareness of our teeth contact prevents tooth loss and TMJ disorder. And it is also related to other body problems like bad posture, stiff neck,
headache, distortion of facial structure, and others. It’s impactful on our daily life situations so it has vital role. Therefore, there is necessity in getting
familiar with our tooth contact because we chew when we’re eating and grind our teeth when sleeping. If your occlusion has a leverage and seesaw
movement, this will gradually damage your teeth and jaw joint. As shown in the figure below, the hinge axis of the jaw joint determines where the lower jaw teeth exactly contact with the upper jaw Teeth. Teeth contact(occlusion) always should not hinder the harmony with the hinge axis of jaw joint !

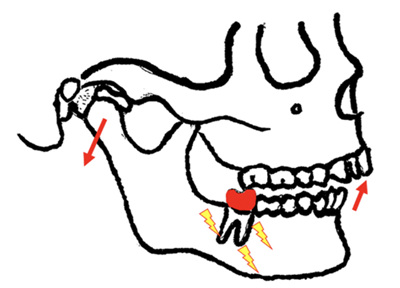
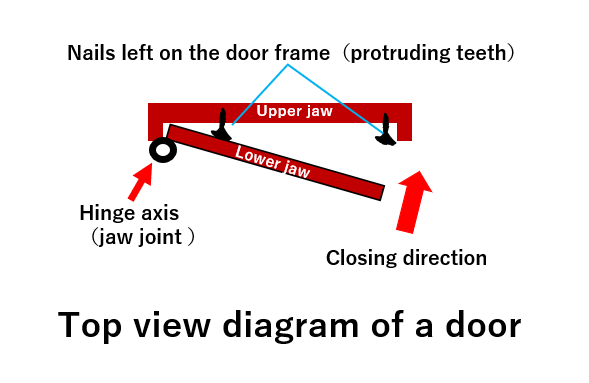
Door hinge analogy for understanding teeth contact so much. When you see the door of a house, think of it as teeth contact.
To better understand it, I created a concept called door hinge analogy. Tooth contact is like the motion of the door in your house. Anything that is
opening and closing has a hinge axis. You can imagine the hinge axis of the jaw joint as the hinge axis of a door, the lower jaw teeth as the door,
while the upper jaw teeth as the door frame. The hinge axis of the door allows the door to open and close smoothly. But if there is a protrusion,
say a nail, near the hinge, the door can’t close smoothly. But not only that, this protrusion becomes a wedge between the door and the door frame
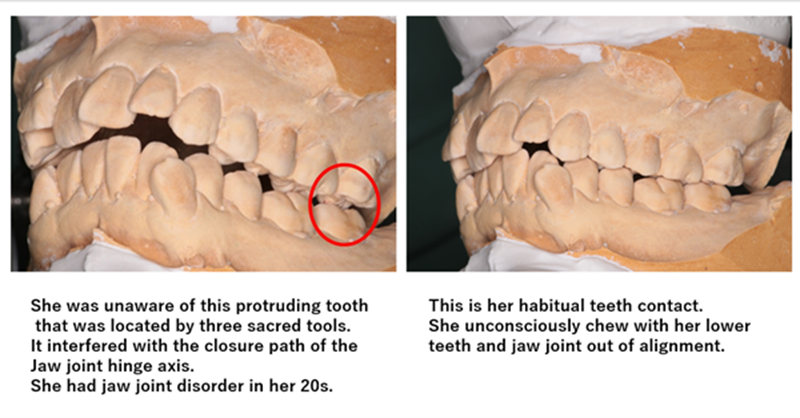
such that when we force it to close, it creates leverage or a see-saw movement that impacts and eventually weakens the hinge axis. The same goes with our dental faculties. If there is a protruding molar tooth, it can hinder the precise contact between the upper and lower incisor teeth during chewing.
This situation will not only cause wear and tear on the molar tooth that could lead to its eventual damage and loss, but it also leads to TMJ disorder.
The solution is to level the protruding molar tooth though shaving. This kind of condition and treatment is the specialty of my clinic.
Anyway, if the protruding tooth is away from jaw joint like an incisor tooth, there is minimal or no impact on the TMJ because it doesn’t create leverage
or a seesaw movement. So, we recommend correcting only the teeth near the jaw joint.
There are only four types of bad occlusion that people are usually not aware of though quite often teeth contact is determined only by your gut feeling and alignment of your front teeth.
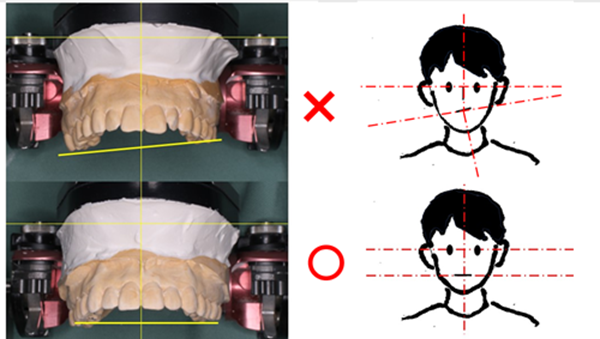
1 . Teeth and jaws are not symmetrically positioned when viewed from the midline.
2. Not all teeth are in contact at the same time.
3. When grinding, molar teeth hit each other.

4. The cusps and fossa of molars are not interlocking contrary to natural teeth formation.
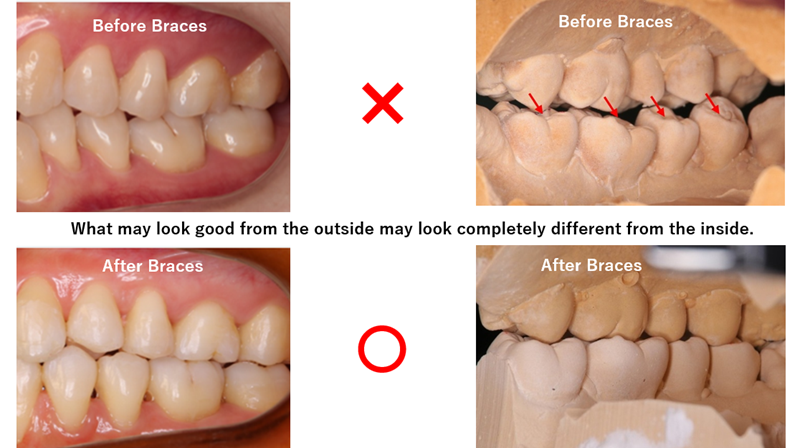
Especially, 2 and 4 lead to tooth loss and jaw joint disorder directly!
Seif-introduction
Hi everyone, I’m Shuichi FUKUNAGA, a Japanese orthodontic doctor running a private clinic in Omiya, Saitama city, Saitama Prefecture. I specialize in occlusion, orthodontic, and oral and maxillofacial surgery. I have worked at the oral and maxillofacial surgery department of a major hospital in Saitama
for more than 30 years. I headed the department before I started my private practice. It was during my stint at the hospital that I’ve specialized in
occlusion and orthodontics for 15years.

